
DVACO-Advance Care Planning Toolkit
Created by: Care Continuum Department & Practice Transformation Team
Date: October 12, 2022
Revised: October 10, 2023
The DVACO has developed an Advance Care Planning (ACP) toolkit compiled of various available resources that can be shared in a customizable way to support providers and to help facilitate goals of care and advance care planning conversations/needs with patients. At any age, a medical crisis could leave a patient too ill to make their own health care decisions. Planning for health care in the future is a major step toward making sure they get the medical care they would want, especially if they are unable to speak for themselves and doctors/family members are making the decisions for them. The resources in this toolkit can aid in the management of the Seriously Ill Populations (SIP), High ED Utilizer, and all other applicable patient populations. Additional forms and resources can be found in the Appendix.
Provider ACP Resources/Information/Documents
The DVACO has compiled a list of below resources to help support and guide healthcare providers in important goals of care conversations.
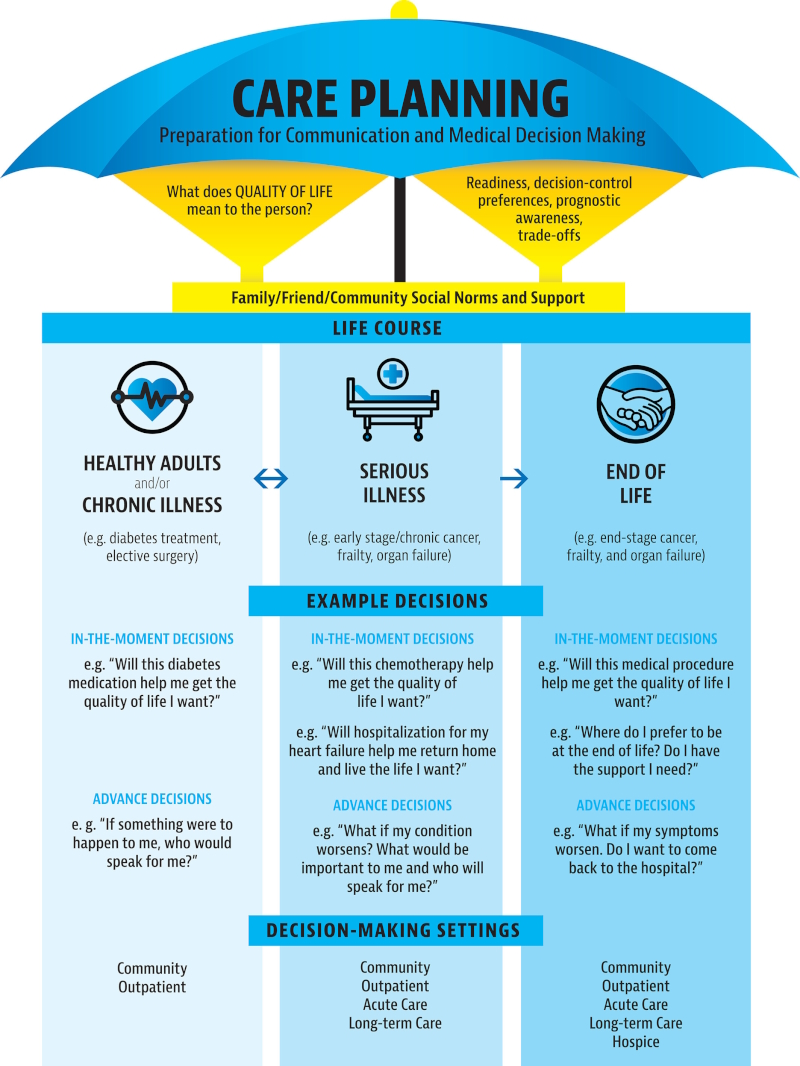
- The care planning umbrella: The evolution of advanced care planning.
Hickman, SE, Lum, HD, Walling, AM, Savoy, A, Sudore, RL. The care planning umbrella: The evolution of advance care planning. J Am Geriatr Soc. 2023; 71(7): 2350-2356.
- CMS-MLN-Advance Care Planning Document
- Serious Illness Conversation Guide
- Condensed Conversation Guide for Identifying Patient Priorities Ambulatory Version
Palliative Care
Palliative care is specialized medical care that treats the symptoms and stress of a serious illness. The goal is to improve quality of life.
- CAPC- Palliative Care Referral Criteria
- MLH-Home Care and Hospice-Choosing the Right Care. – Palliative care is specialized medical care for patients at any stage of serious illness regardless of receiving curative medical treatment. Hospice care is comfort care at end-of-life when curative is no longer beneficial or desired.
- Co-Management Home-Based Palliative Care Service Providers – A list of vetted in-home palliative care providers in the Philadelphia region to help support caregivers and patients with serious illness.
Physician Orders for Life-Sustaining Treatment (POLST)
The POLST is specifically designed to document an individual’s treatment choices for end-of-life care whether the choice is for resuscitation or no resuscitation. POLST orders also extend to addressing choices for full or limited medical treatment or comfort measures only. It is designed to be portable, travel with the patient and be respected in multiple care settings.
- Pennsylvania’s Out-of-Hospital Do-Not-Resuscitate Order and Physician Orders for Life-Sustaining Treatment Similarities and Differences
- Appropriate Use of POLST
Patient ACP Resources/Information/Documents
Goal-focused care is pursued through advance care planning. This helps patients (or their surrogate medical decision maker) understand their diagnosis, prognosis, and treatment options. ACP involves shared decision making to ensure that health care professionals make care recommendations that are sensitive to what matters most to patients, and that patients and surrogates always have the opportunity to make informed care decisions.
- Patient Conversation Starter Guide – a digital guide for patients on how to identify their goals of care that can be shared with their medical providers and caregivers.
- PREPARE-Patient Pamphlet – a patient pamphlet to guide a patient’s thought process for medical decisions
- Who Needs a POLST, a Portable Medical Order?
ACP Billing
Advance care planning is to be completed at the patient’s discretion. Medicare waives the ACP deductible and coinsurance once per year when billed with the AWV. The deductible and coinsurance apply when you give the ACP outside of the covered AWV. There are no limits on the number of times you can report ACP for a given patient in each time period. When billing this patient service multiple times, ensure you are updating and documenting the changes in the medical record.
If the patient would like to complete ACP, the following should be included in the conversation and documented:
- Any future care decisions that may be needed
- How the patient can share the information with others
- Identification of the caregiver
- Explanation of Advance Directives
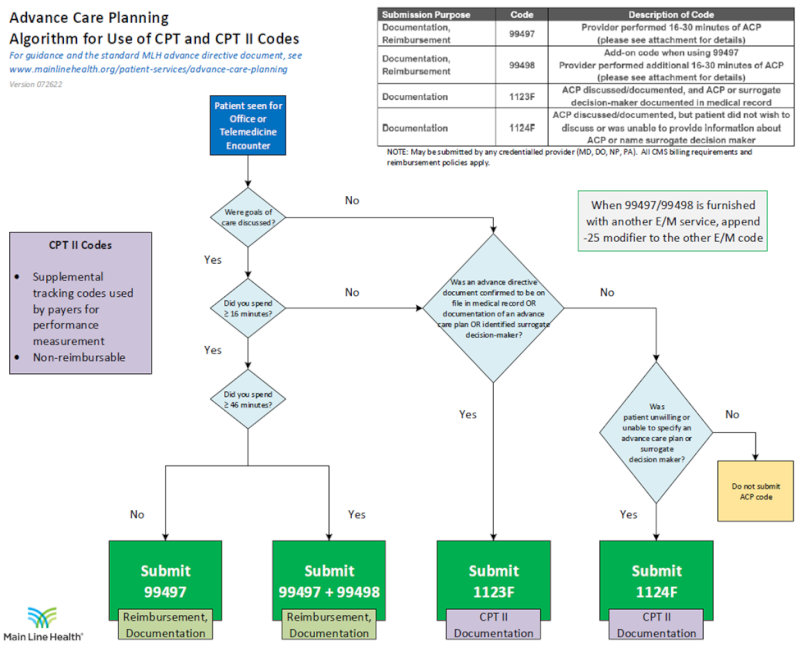
If the patient declines ACP, the provider can submit CPT II code 1124F. CPT II codes are supplemental tracking codes ($0 billable charge) that can be used by providers to submit specific information to a payer that will relay information about health information or health outcomes that ICD-10 codes or CPT I codes cannot.
Billing Advance Care Planning during an AWV
Use the following CPT codes when billing for Advance Care Planning during the AWV:
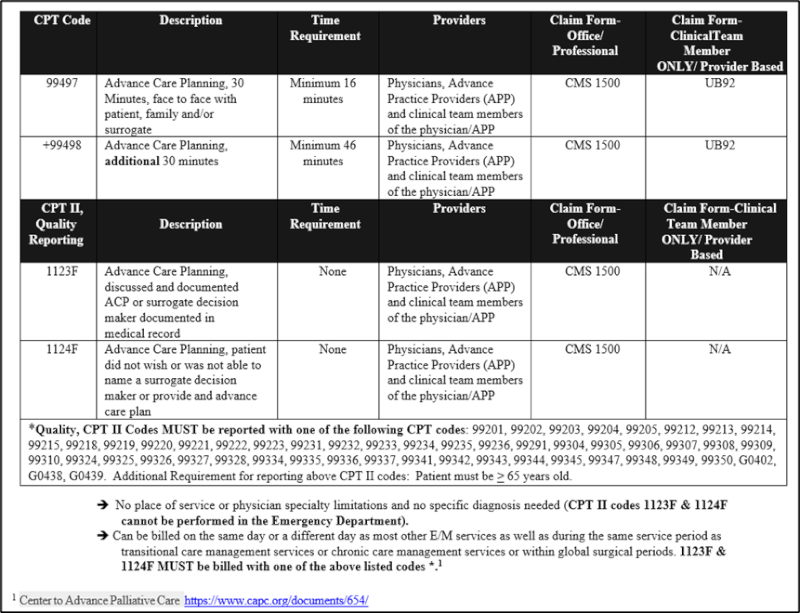
- 99497- Advance care planning including the explanation and discussion of advance directives such as standard forms (with completion of such forms, when performed), by the physician or other qualified health care professional; first 30 minutes, face-to-face with the patient, family member(s), and/or surrogate
- 99498- Advance care planning including the explanation and discussion of advance directives such as standard forms (with completion of such forms, when performed), by the physician or other qualified health care professional; each additional 30 minutes (List separately in addition to code for primary procedure)
Medicare waives both the ACP coinsurance and the deductible if:
- Given on the same day as the covered AWV
- Given by the same provider as the covered AWV
- Billed with modifier –33 (Preventive Service)
- Billed on the same claim as the AWV
Additional Online On-demand Educational Opportunities
- Institute for HealthCare Improvement: IHI Open School Online Curriculum
- PFC 202: Having the Conversation: Basic Skills for Conversation about End-of-life Care.
- PFC 203: Providing Age-Friendly Care to Older Adults
- Center to Advance Palliative Care- Contact DVACO for CAPC login information
- Patients & Guests – Advance Directive | Jefferson Health
- Jefferson Advance-Directives-English
- Jefferson Advance-Directives-Spanish
- MLH-Advance-Care-Planning-Process
- PA DOH ACP Documents – Living Will & Healthcare POA
- PA DOH-ACP- English Stand-Alone Form (no directions)
- PA DOH-ACP-Spanish Version Stand Alone Form (no directions)
- PA DOH- Introduction to the POLST Form
- PA DOH- Introduction to the POLST Form (Spanish Version)
- NJ Durable Power of Attorney for Health Care
- NJ Instruction Directive (Living Will)
- NJ-POLST Form
https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNProducts/MLN-Publications-Items/ICN909289
https://www.capc.org/
https://www.health.pa.gov/
https://www.ihi.org/
https://www.papolst.org/pa-polst-form